On April 18th I attended the London Region
conference for the RCN safe staffing campaign. I was surprised at how small the
conference was, with only 30-40 spaces for members to attend when RCN London's membership is well over 60,000.
Still it was a promising initiative that showed
the RCN leadership is trying to do things differently and move away from the
top down approach of running things that has exemplified their campaigns for
the last several years.
There was an introduction from officers, and from lay members like activist Michael Coram, laying out how the RCN was going to combine ideas from the safe staffing conferences, professional bodies, the trade union caucus, RCN officers and the council to develop the campaign. The regional conference were to tap the experiences and thoughts of lay members and to feed them in to the process.
There has been a glaring need for an active RCN
safe staffing campaign for years. Frustratingly the chance to organise one
after the Mid Staffs scandal and outcome of the Francis Inquiry was frittered
away by the conservative RCN leadership.
Now the RCN is taking this more bottom up
approach this offers a real opportunity for nurses to organise a radical, ward-nurse
lead safe staffing campaign that can secure the immediate improvements we need
in staffing levels across the NHS.
After the discussion of how the different parts
of the RCN would have input in to the campaign’s development, we undertook
several group exercises to develop our own ideas about what constituted safe
staffing, and what ways we would communicate this to the public. This
encouraged wide ranging discussion as different perspectives and experiences
were put forward on what was considered safe and unsafe staffing, and how this
impacted on patient and nurse wellbeing. We wrote down our ideas and each group
presented them to the conference, encouraging further debate.
Ward nurses talked about being constantly under
pressure and patients never feeling safe, while community nurses talked about
workloads which were impossible to meet with understaffed community services.
Students described being unable to find time for teaching, and having to in
effect work as HCAs, or even effectively as nurses because there were not
enough staff on the wards to do all the work. Comp[arisons were made with other
services, like airlines where planes can’t fly without enough crew, and how
there isn’t the same level of enforced safety in many hospitals and services.
There
were too many different ideas and ways of communicating them brought forward
for me to record them all here, and it highlighted the potentially vibrant
atmosphere that could be created if nurses doing the work on the ground were
given input in to or put in charge of how we developed and communicated our
message.
I argued repeatedly that we needed to focus on
mandatory staffing ratios as the aim of the campaign, and should model our
activism on what had gotten results in California and Australia, the two places
where nurses have won mandatory nurse:patient ratios through militant campaigns
lead by nursing unions. This was taken up by some, but others were opposed or
not convinced yet, while some nurses working in the community spoke of how they
needed other ways of calculating safe staffing as their services and patient
caseloads worked differently.
We then looked at different logos and slogans
the RCN was proposing for use in the campaign. We wrote down our thoughts on
what the images represented, their strengths and weaknesses, and what they
might represent to us or the public. Previous regional gatherings had developed
the hashtag #safestaffingsaveslives, and the slogan Safety in Numbers was
popular in the London conference.
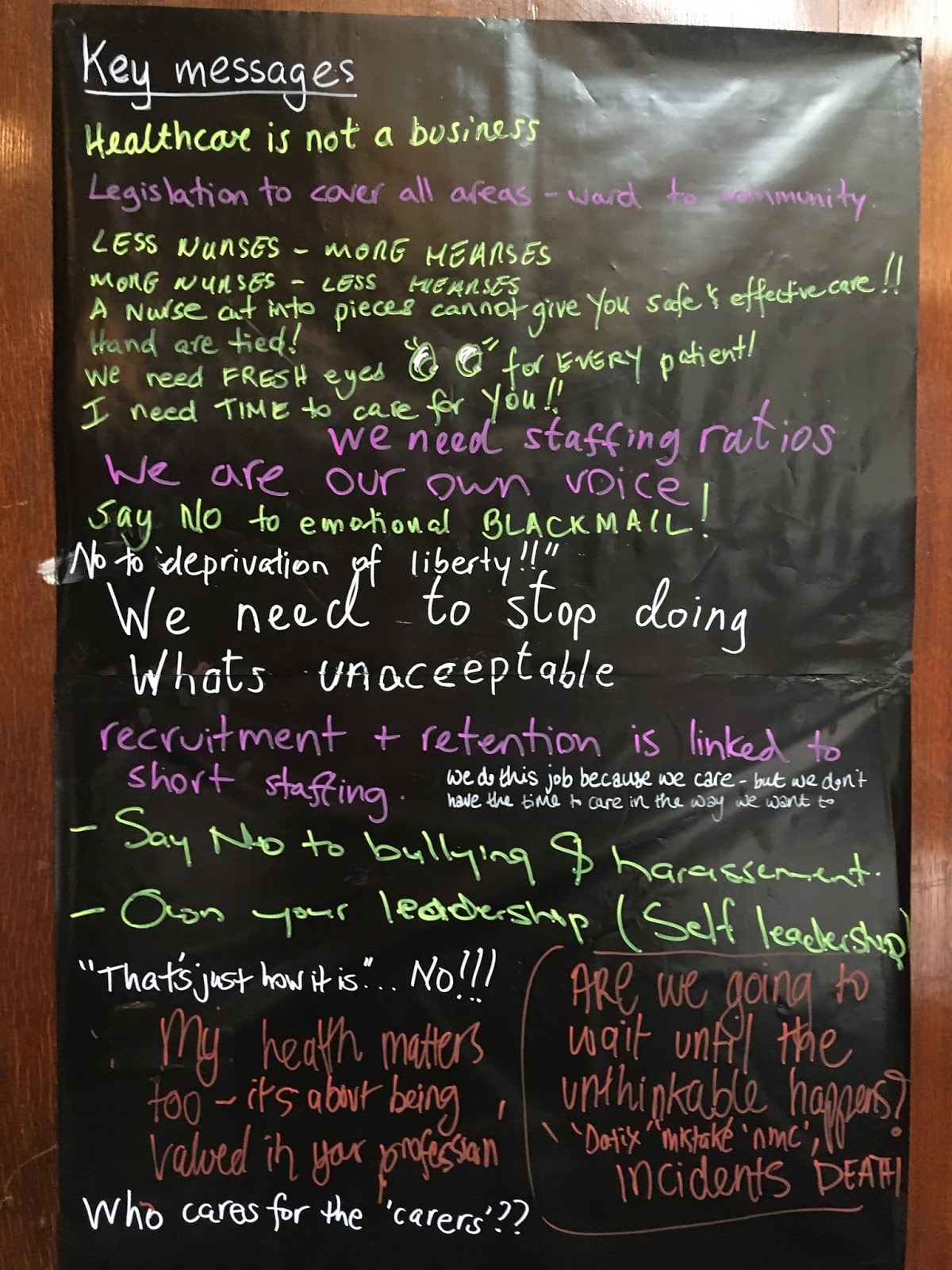
After this we undertook an exercise where we wrote our ideas on large sheets of card stuck to the walls of the meeting room. We were asked to write slogans, images and other things which we thought the campaign should include. Pictures of the boards are below:


During this process we were told more about what the focus of the campaign was and what RCN officers saw as its aim. The inspiration for the campaign was partly the enormous nurse staffing crisis, and partly the passing of the Nurse Staffing Levels (Wales) Act 2016 by the Welsh Assembly. This was the culmination of years of campaigning by the RCN and several Welsh assembly members. RCN officers stated the present aim of the campaign would be to bring in a similar law in the NHS in England, and other devolved nations.
The effect of the Welsh act was to make several more members of the Hospital board responsible for safe staffing. It “introduces a duty for Local Health Boards and NHS Trusts in Wales (where applicable) to calculate and take all reasonable steps to maintain nurse staffing levels and inform patients of the level.” Currently, only a Chief Nurse is responsible for staffing levels, and as of writing, no Chief Nurses have yet been held accountable for poor nurse staffing taking place at their Trust, despite their direct responsibility for the matter. The law does not stipulate what nurse staffing levels should be, and the process for calculating what that is based on the same overly complex and flawed system of patient acuity tools and professional judgement that operates presently. The system leaves far too much leeway for hospital managers to alter staffing levels to suit their budgeting needs, rather than what is safest for patients.
The legal change and its impact would be
relatively small. A similar law implemented in England would make four officers
of the Trust board (Chief Executive, Chief Finance, Chief Operations and Chief
Nurse) responsible for staffing, as opposed to just one at present, the Chief
Nurse. One RCN officers stated that in Wales the change had not lead to any
noticeable improvement in staffing levels or nurse:patient ratios, rather it
had only made trust management reluctant to cut nurse staffing budgets as more
of them would be held accountable for the results. While anything which reduces
cuts to staffing budgets is welcome, this is not the radical and wide ranging
change we need, and all the signs are it would not secure us the immediate
improvement in our staffing situation that we need to avert the collapse of
nursing and the NHS.
When RCN officers were asked about whether
securing this tweaking of legal responsibility for safe staffing really went
far enough, and really reflected the full potential of ideas and energy present
in the room, the response was the campaign was open to influence by the members
and its final form would not be decided till conference.
It was welcome to hear this, but it shows that
RCN members who want a radical campaign for safe staffing levels are going to
have to work hard and get involved in the campaign to change it in to what we
want it to be.
If left up to RCN officers, we will be left with
a campaign narrowly focused on securing a change in legal responsibility for
ensuring safe staffing. This would not change the situation on the wards or in
the community, where the vast majority of nurses work. To put all the efforts
of our hundreds of thousands of members in to securing this small legal change
would be a waste of the potential energy and commitment available.
It is also important to note who this legal
change would benefit. Taking part in the conference were several heads of
nursing and directors of nursing. When myself and other activists raised the
idea of campaigning for mandatory nurse:patient ratios to improve staffing
levels, these members were the most outspoken in opposing the idea. They were
however in favour of securing the legal change as outlined in the Welsh act.
Why the opposition to staffing ratios, but support for increased legal
responsibility?
The reason should be clear; making more managers
responsible for staffing makes it easier for nurse managers to protect their
budgets, it empowers them in their arguments over allocating scare NHS
resources. What it won’t do is secure us a significant improvement in staffing
levels, or the increased investment to pay for that.
As has been shown by nurses in California and
Australia, only when nurses fight for legally enforced, mandatory minimum
nurse:patient ratios are hospital management forced to employ enough nurses to
staff wards properly. With the legal duty to employ a certain ratios of nurses
to patients, government and private hospital corporations can be compelled to
provide the funding to pay for it. When staffing is left up to senior managers,
the needs of the budget and either government finances or private profit come
before patient care.
For the last six years we have had hospital
management and government budget constraints determining nurse staffing levels,
and it has resulted in the terrible situation we are in now. We cannot waste
this opportunity to go further with the campaign and secure mandatory minimum
safe staffing levels across the NHS.
Activists should take the lead in convening meetings in their hospitals and community services to discuss the staffing campaign and start getting RCN members involved in campaigning. Activists and reps should get members to decide on their priorities for their hospital, branch and region and feed that back in to the campaign. The more ward nurses are involved agitating and arguing for mandatory staffing ratios, the more that message will come through in the campaign.
The more organised we are in our workplaces, the more we can influence the campaign and ensure the it develops in the radical direction it needs to secure the changes we need.
Activists should take the lead in convening meetings in their hospitals and community services to discuss the staffing campaign and start getting RCN members involved in campaigning. Activists and reps should get members to decide on their priorities for their hospital, branch and region and feed that back in to the campaign. The more ward nurses are involved agitating and arguing for mandatory staffing ratios, the more that message will come through in the campaign.
The more organised we are in our workplaces, the more we can influence the campaign and ensure the it develops in the radical direction it needs to secure the changes we need.
Below I’ve outlined some of the shortcomings of
previous safe staffing campaigns by the RCN, and the lessons to be learned from
them.
Lessons from the Safe Staffing Alliance
After the Francis Report was published, when the
RCN leadership should have used the widespread anger and horror at the Mid
Staffs scandal and the Francis Report to mobilise the RCN membership and the
public to lobby the government and NHS institutions for change, what resulted
from the scandal was a limited campaign aimed at softly lobbying NHS policy
makers through articles in the media and publicising safe staffing research.
Called the Safe Staffing Alliance, the
campaign was organised with UNISON, the Patients Association, the Florence
Nightingale foundation and the Nursing Standard. The Safe Staffing Alliance
focused on changing the minds of ministers and NHS board members using the well
documented evidence that higher nurse staffing levels are vital for good
patient care.
It held roundtables
and produced a manifesto,
press releases, and a leaflet,
but made no attempt to organise nurses in hospitals to campaign for better
staffing themselves. Instead the task was left up to the academics and senior
policymakers from think tanks who would speak to senior NHS managers and
convince them of the need for better nurse staffing.
In short, this approach failed. Despite being
set up in January 2013, the campaign produced no significant changes in nurse staffing
levels. The campaign gave input in to the research on staffing levels by NICE, (started
after the Francis report) that was beginning to result in policy outlining
staffing ratios for acute hospitals. When this research was halted by Jeremy
Hunt and NHS England the campaign became inactive. The last statement on their homepage
is in reference to the cancellation of NICE research in 2016, asking nurses to
sign up to the campaign, but proposing no concrete action to lobby the
government to restart the research.
The campaign’s demands were incredibly minimal in themselves, calling for “Never more than 8”, so wards should have no more than 8 patients per nurse, and if this occurred, for it to be recorded as an safety incident. While the campaign called for this to be a floor, rather than a ceiling, it quickly became the ceiling where hospitals could afford to meet it. In many that couldn’t it remained just an aspiration. The campaign did not call for any legal measures to enforce this staffing level, just relying on nurse managers and acuity-based staffing tools to enforce effective staffing levels.
The campaign’s demands were incredibly minimal in themselves, calling for “Never more than 8”, so wards should have no more than 8 patients per nurse, and if this occurred, for it to be recorded as an safety incident. While the campaign called for this to be a floor, rather than a ceiling, it quickly became the ceiling where hospitals could afford to meet it. In many that couldn’t it remained just an aspiration. The campaign did not call for any legal measures to enforce this staffing level, just relying on nurse managers and acuity-based staffing tools to enforce effective staffing levels.
This approach was blind to the reality of the
impact of austerity on the NHS, and why nurse staffing remains a contentious
issue and has not been “solved” despite the mountains of evidence and policy
demonstrating its importance to good patient care.
Nurses have always been the largest single group of staff in any hospital or health service. They perform the key practical tasks of patient care and treatment whether in hospitals or community services and so there need to be lots of them. Conversely, this means when budgets are frozen or cut, finance managers look to make savings on their biggest outgoing, nurse salaries. When the NHS budget was frozen under the Cameron government, managers enforced vacancy freezes and downgraded and cut nursing posts to try and balance their budgets.
This was the context when the Francis Report was published; frozen budgets and no new investment. For this reason, no appeals to the reasons and understanding of senior NHS managers could work; they were tasked with balancing their budgets and holding costs down, while safe nurse staffing required a large injection of funding and staff. Alongside the financial pressures, the only effective measure to increase staffing levels - mandatory minimum staffing levels - was opposed by the government as it would set in stone staffing levels preventing management’s ability to carry out cuts and reduce the NHS budget, and it would disempower senior managers and empower ward level nurses to an unacceptable degree.
So while the Francis Report lead to small improvements in transparency, such as hospitals and wards recording and publicising their staffing levels, it created no fundamental change in how staffing was organised; it was still determined by senior NHS hospital managers on the basis of what could be afforded, rather than what was necessary for good patient care. Despite all the lobbying of NHS decision makers by the Safe Staffing Alliance, despite all the evidence from researchers and policy makers, the staffing situation is now as bad as it ever was, but with the added complication of the nurse recruitment and retention crisis that has developed as a result of chronic understaffing driving thousands of nurses to leave the profession.
Nurses have always been the largest single group of staff in any hospital or health service. They perform the key practical tasks of patient care and treatment whether in hospitals or community services and so there need to be lots of them. Conversely, this means when budgets are frozen or cut, finance managers look to make savings on their biggest outgoing, nurse salaries. When the NHS budget was frozen under the Cameron government, managers enforced vacancy freezes and downgraded and cut nursing posts to try and balance their budgets.
This was the context when the Francis Report was published; frozen budgets and no new investment. For this reason, no appeals to the reasons and understanding of senior NHS managers could work; they were tasked with balancing their budgets and holding costs down, while safe nurse staffing required a large injection of funding and staff. Alongside the financial pressures, the only effective measure to increase staffing levels - mandatory minimum staffing levels - was opposed by the government as it would set in stone staffing levels preventing management’s ability to carry out cuts and reduce the NHS budget, and it would disempower senior managers and empower ward level nurses to an unacceptable degree.
So while the Francis Report lead to small improvements in transparency, such as hospitals and wards recording and publicising their staffing levels, it created no fundamental change in how staffing was organised; it was still determined by senior NHS hospital managers on the basis of what could be afforded, rather than what was necessary for good patient care. Despite all the lobbying of NHS decision makers by the Safe Staffing Alliance, despite all the evidence from researchers and policy makers, the staffing situation is now as bad as it ever was, but with the added complication of the nurse recruitment and retention crisis that has developed as a result of chronic understaffing driving thousands of nurses to leave the profession.
We cannot adopt the same campaigning approach
again. We have to learn from where safe staffing ratios have been won before,
and replicate their tactics and strategies.
What has worked is militant trade union campaigns,
seeking to organise nurses in the workplace to take industrial action through
protests and strikes, forcing management to take action on the issue. Workplace
organizing was combined with public demonstrations and protests pushing the
government to legislate for safe staffing, mobilizing the high levels of public
support for nurses and everyone’s interest in securing a safer healthcare system. In Australia nurses taking strike action won ratios back in 2000 as part of their collective bargaining agreement with the government. These ratios covered all public hospitals. In California ratios were implemented in 2004 after a three year campaign.
It has now been six years since the Francis report. If the RCN had
adopted a more militant and active campaigning approach in 2013, we could very well have secured staffing ratios
by now in the UK.
Anyone interested in learning about how nurses
won ratios in other parts of the world should read Safety
in Numbers: Nurse-to-Patient Ratios and the Future of Healthcare. This is
an excellent academic study of how the ratio campaigns developed in America and
Australia, and it deals with many of the misunderstandings and misconceptions
about how staffing ratios work. I highly recommend every nurse activist buys
and reads the book.
The California Nurses Association/National Nurses United have published this booklet The Ratio Solution making the case for ratio legislation, and tackling the hard questions of how they will work. Implementing ratios reversed a decline in nurse numbers taking place in California very similar to our own, and there were 100,000 more RNs in service within 10 years of the law being enacted.
The Australian Nursing and Midwifery Federation Victoria Branch has produced this booklet Nurse/Midwife: Patient Ratios outlining the benefits of ratios. They were so successful in Australia in improving patient safety and workplace conditions that the government passed them in to law in 2015.
Draft motion for branches
I am proposing this motion to my RCN branch, please feel free to adopt and adapt and submit it to your own branch.
For a militant campaign for mandatory staffing levels
This branch notes
1. A new study has shown that 1 in 4 NHS wards were staffed at dangerous levels, and that understaffing of wards remains widespread, despite the impact of the Mid Staffs enquiry, repeated concerns raised by nursing unions and academics, and the limited work done on safe staffing by NICE.
2. These figures reflect that little has changed since the Mid Staffs enquiries, and a new approach to tackling unsafe staffing must be made by the RCN.
3. This failure to tackle the understaffing crisis is leading to the decimation of the nursing profession, with more nurses leaving than joining the register in 2017 and 2018.
4. That there are currently 40,000 nursing vacancies in the NHS, and this is projected to rise to 100,000 over the next decade.
This branch believes
1. There is strong evidence that energetic and militant campaigns by nursing unions have won mandatory staffing levels that have benefited patients and nurses.
2. Both the California Nurses Association/National Nurses United, and the Australian Nursing and Midwifery Federation have achieved mandatory safe staffing levels in law and collective agreements by mobilising their members in protests, and being prepared to take strike action to achieve their goals
3. That the RCN must learn from and copy these approaches if it is to achieve safe staffing legislation in the UK.
4. That the mandatory minimum staffing ratios developed by CNA/NNU and the ANMF are good examples to follow, and the RCN should adopt similar clear demands for mandatory staffing ratios as part of its campaign.
5. That urgent action is needed to advance the campaign and secure an improvement in nurse staffing levels across the NHS.
This branch calls for
1. The RCN to learn from the CNA/NNU and ANMF and advance their militants tactics for the safe staffing campaign; organising regular public protests and demonstrations, and being prepared to take strike action to secure safe staffing levels.
2. The RCN to adopt a ratio based approach for safe staffing levels, developing its own staffing ratios and putting them forward as part of its demands for safe staffing legislation.
3. Organising regular protests at the Department of Health to raise the profile of the safe staffing campaign, to maintain pressure on the government throughout the campaign, and that branches can and should take the lead in organising these protests.
4. A protest to be organised within the next three months at the Department of Health calling for mandatory minimum staffing ratios to be implemented in the NHS. We invite other London branches, and the London Board to support and publicise this initiative.
When passed, please submit the motion to your regional Board and to RCN Council to show support for campaigning for staffing ratios.
Draft motion for branches
I am proposing this motion to my RCN branch, please feel free to adopt and adapt and submit it to your own branch.
For a militant campaign for mandatory staffing levels
This branch notes
1. A new study has shown that 1 in 4 NHS wards were staffed at dangerous levels, and that understaffing of wards remains widespread, despite the impact of the Mid Staffs enquiry, repeated concerns raised by nursing unions and academics, and the limited work done on safe staffing by NICE.
2. These figures reflect that little has changed since the Mid Staffs enquiries, and a new approach to tackling unsafe staffing must be made by the RCN.
3. This failure to tackle the understaffing crisis is leading to the decimation of the nursing profession, with more nurses leaving than joining the register in 2017 and 2018.
4. That there are currently 40,000 nursing vacancies in the NHS, and this is projected to rise to 100,000 over the next decade.
This branch believes
1. There is strong evidence that energetic and militant campaigns by nursing unions have won mandatory staffing levels that have benefited patients and nurses.
2. Both the California Nurses Association/National Nurses United, and the Australian Nursing and Midwifery Federation have achieved mandatory safe staffing levels in law and collective agreements by mobilising their members in protests, and being prepared to take strike action to achieve their goals
3. That the RCN must learn from and copy these approaches if it is to achieve safe staffing legislation in the UK.
4. That the mandatory minimum staffing ratios developed by CNA/NNU and the ANMF are good examples to follow, and the RCN should adopt similar clear demands for mandatory staffing ratios as part of its campaign.
5. That urgent action is needed to advance the campaign and secure an improvement in nurse staffing levels across the NHS.
This branch calls for
1. The RCN to learn from the CNA/NNU and ANMF and advance their militants tactics for the safe staffing campaign; organising regular public protests and demonstrations, and being prepared to take strike action to secure safe staffing levels.
2. The RCN to adopt a ratio based approach for safe staffing levels, developing its own staffing ratios and putting them forward as part of its demands for safe staffing legislation.
3. Organising regular protests at the Department of Health to raise the profile of the safe staffing campaign, to maintain pressure on the government throughout the campaign, and that branches can and should take the lead in organising these protests.
4. A protest to be organised within the next three months at the Department of Health calling for mandatory minimum staffing ratios to be implemented in the NHS. We invite other London branches, and the London Board to support and publicise this initiative.
When passed, please submit the motion to your regional Board and to RCN Council to show support for campaigning for staffing ratios.
No comments:
Post a Comment